Your Body Is Talking — Learn to Listen
A dull shin on a Tuesday morning, the five injuries that ambush almost half of all runners, and the four-level framework for deciding whether to lace up or rest.
It's week five of your training plan. You wake up on a Tuesday morning, swing your legs out of bed, and feel a dull ache along the inside of your right shin. You limp to the bathroom, but by the time you've showered it's barely noticeable. Your training schedule says four-mile easy run today. So what do you do?
If you're like most beginning runners, you face this kind of question at least once during training, and how you answer it will likely determine whether you make it to the start line. Injury is the number-one reason people abandon marathon training, and the cruel irony is that most of those injuries were preventable. They started as whispers. The runners who quit were the ones who didn't know how to hear them, or who heard them and chose not to listen.
An Uncomfortable Truth
Let's start with an uncomfortable truth: running injuries are staggeringly common. A systematic review of forty-two studies by Kakouris and colleagues in 2021 found an overall injury incidence of forty point two percent among runners, with a prevalence reaching forty-four point six percent. That means nearly half of all runners are dealing with an injury at any given time. Among the studies examining overuse injuries specifically, the numbers are even more striking. According to Taunton and colleagues in 2012, up to seventy percent of runners sustain an overuse injury annually.
But here's the number that should give you hope: the vast majority of these are OVERUSE INJURIES, not sudden accidents, not freak occurrences, but the accumulated result of repetitive stress exceeding your body's capacity to recover. And overuse injuries almost always announce themselves before they become serious. The shin that aches for a minute after a run. The knee that feels off going downstairs. The heel that's stiff for the first ten steps of the morning. These aren't random events. They're your body's early warning system, and this chapter is about learning to decode the messages.
The Adaptation Gap, Revisited
In Chapter Two, we introduced a concept that becomes absolutely critical now: the CARDIOVASCULAR-MUSCULOSKELETAL ADAPTATION GAP. Your heart and lungs adapt to training stress relatively quickly. Within days to weeks, you'll notice that runs feel easier, your breathing is more controlled, and your resting heart rate drops. This cardiovascular fitness improvement feels wonderful, and it's dangerously seductive.
Your musculoskeletal system, bones, tendons, ligaments, cartilage, and the connective tissue wrapping your muscles, adapts on a completely different timeline. Tendons may take weeks to months to strengthen. Bone remodeling operates on a cycle of roughly three to four months. This means there's a window, often between weeks three and eight of a new training program, where your cardiovascular fitness outpaces your structural resilience. You feel ready to run farther and faster. Your bones and tendons are not.
Taunton and colleagues in 2012 identified this gap as a primary explanatory framework for why overuse injuries occur in runners. It's not that running is inherently dangerous. It's that runners consistently outrun their body's structural readiness, precisely because their cardio system is telling them they can. Understanding this gap is the single most important concept in injury prevention.
Discomfort Is Not Pain
Marathon training is uncomfortable. That's not a flaw in the process, it IS the process. Your body adapts to stress by rebuilding stronger, and that rebuilding involves inflammation, micro-repair, and the general sensation of muscles that have been asked to do more than usual. Learning to tolerate this productive discomfort is a fundamental part of becoming a runner.
But, and this is the critical distinction, discomfort and pain are not the same thing. Discomfort is diffuse, bilateral on both sides, fades during activity, and resolves within hours. Pain is specific, often unilateral on one side, worsens during or after activity, and persists or returns. Confusing the two leads runners into one of two traps: either they stop at every minor sensation and never build fitness, or they push through genuine warning signs and end up injured.
Normal adaptation includes general muscle soreness that appears twenty-four to forty-eight hours after a harder effort, what we call delayed-onset muscle soreness, or D-O-M-S. It includes bilateral symptoms, both calves feel tight, both quads are heavy. This normal discomfort improves with gentle movement. The stiffness fades after a warm-up. It resolves within forty-eight to seventy-two hours without intervention, and crucially, it has no impact on your running form. You might be slower, but your gait feels normal.
Reading the Body Map
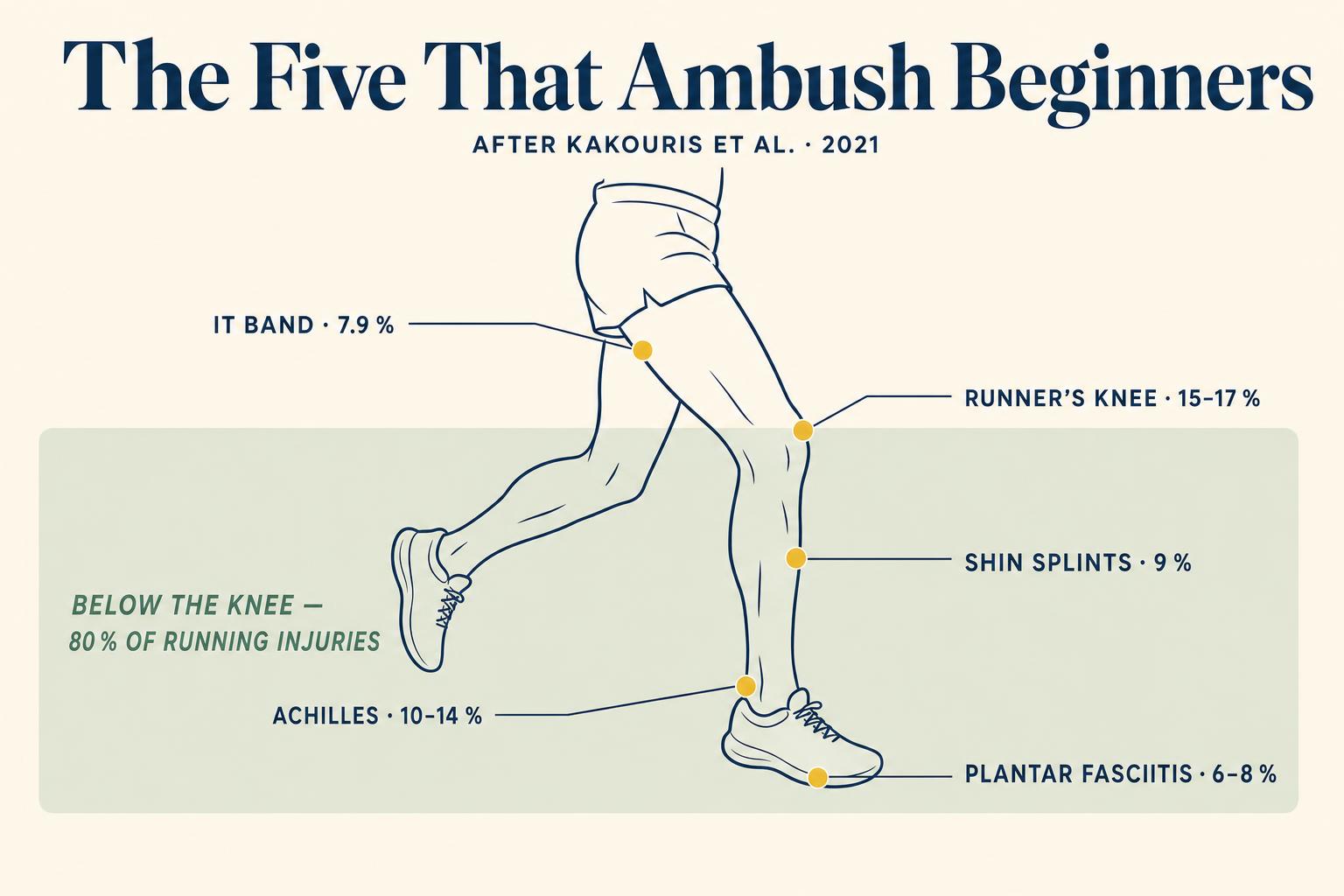
First, RUNNER'S KNEE, also called patellofemoral pain syndrome. It feels like a dull, aching pain around or behind the kneecap, worst when going downstairs, sitting for long periods, or during the early miles of a run. The prevalence is fifteen point eight to sixteen point seven percent of all running injuries according to Kakouris and colleagues. It usually happens from a combination of weak hip stabilizers, especially the gluteus medius, and increased training load. When your hip drops during each stride, your knee compensates with poor tracking of the kneecap. The early warning is knee stiffness after sitting that resolves within a few steps, a vague sense that your knee doesn't feel right on descents.
Second, SHIN SPLINTS, medically called medial tibial stress syndrome. Pain along the inner edge of the shinbone, often over a broad area rather than one point. Prevalence is nine point one to nine point four percent. It happens because the tibial bone is remodeling in response to the new impact loads of running, but you're adding stress faster than remodeling can keep up. This is the adaptation gap in its purest form. The early warning is shin tenderness that appears after runs and disappears by the next day. If it starts appearing during runs or becomes point-specific, the situation is escalating.
Third, ACHILLES TENDINOPATHY. Stiffness and pain in the Achilles tendon, that thick cord at the back of your ankle, especially in the first few minutes of walking after rest. Prevalence is ten point three to thirteen point seven percent. Tendons adapt slowly to load, and the Achilles bears enormous force during running, up to six to eight times your body weight with each stride. Sudden increases in speed work or hill running are common triggers. Early warning includes morning stiffness in the tendon that resolves within the first five to ten minutes of movement, a creaky feeling at the start of runs.
Fourth, PLANTAR FASCIITIS. A sharp, stabbing pain under the heel or along the arch, worst with the first steps of the morning. Prevalence is six point one to seven point nine percent. The plantar fascia, a thick band of tissue on the bottom of your foot, becomes irritated from repetitive loading. Higher B-M-I, body mass index, tight calves, and rapid mileage increases are risk factors. The early warning is a mild ache in the heel at the end of longer runs, or slight stiffness in the arch first thing in the morning.
Fifth, I-T BAND SYNDROME, or iliotibial band syndrome. A sharp, burning pain on the outside of the knee, usually appearing at a specific point during a run, often around fifteen to twenty minutes in, and worsening until you stop. Prevalence is seven point nine percent. The iliotibial band, a thick strip of connective tissue running from hip to knee, compresses a fat pad on the outside of the knee during repetitive flexion and extension. Weak hip abductors and downhill running are common contributors. The early warning is a subtle tightness on the outer knee that resolves when you stop running, only to appear slightly earlier in your next run.
Notice that all five injuries share a common theme: they develop gradually and have recognizable early warning signs. The patterns across these injuries show that weak stabilizing muscles, rapid increases in training load, and the mismatch between cardiovascular fitness and structural readiness all play critical roles.
Strength, Not Stretching
If there's one evidence-backed intervention that deserves your attention as a new runner, it's STRENGTH TRAINING, and not the kind you might be imagining. We're not talking about bodybuilding or heavy squats, though those aren't harmful. We're talking about targeted exercises for your glutes, hips, and core, the stabilizing muscles that control how your leg absorbs impact with every stride.
Blagrove and colleagues in 2022 conducted a comprehensive narrative review showing that lower-limb resistance exercise improves running economy and may help reduce injury risk. The mechanism is straightforward: stronger stabilizers mean better control of the knee and ankle during the repetitive motion of running, which reduces the abnormal loading patterns that cause overuse injuries. A combination of strength and plyometric training appears to offer the greatest benefit.
However, and this is an important nuance, a subsequent meta-analysis by Blagrove and colleagues in 2024 found that exercise-based prevention programs don't consistently reduce injury rates overall. The critical caveat? Supervised interventions showed significantly lower injury risk compared to controls. The exercises themselves work; the challenge is doing them correctly and consistently. This is why learning proper form matters, and why a few sessions with a physiotherapist or strength coach can be a worthwhile investment.
A basic runner's strength routine doesn't require a gym membership or an hour of your time. Fifteen to twenty minutes, two to three times per week, focusing on these movement patterns, will provide substantial benefit. Single-leg glute bridges target the gluteus maximus, the primary hip extensor in running. Clamshells or side-lying hip abduction strengthen the gluteus medius, preventing the hip drop that contributes to runner's knee and I-T band issues. Single-leg calf raises build Achilles tendon capacity and protect against Achilles tendinopathy and plantar fasciitis. Copenhagen planks or side planks address hip adductor strength and core stability. Step-downs or single-leg squats integrate hip and knee control in a functional movement pattern.
Three Honest Words About Three Things
Now let's address three topics that generate enormous confusion among new runners. First, STRETCHING. The belief that stretching prevents running injuries is one of the most persistent myths in recreational fitness. While flexibility has its place, the research consistently fails to show that pre-run static stretching reduces injury risk. In fact, static stretching before a run can temporarily reduce muscle force production. Dynamic warm-ups, leg swings, walking lunges, high knees, are a better choice before running. Save static stretching for after your run if it feels good, but don't rely on it as injury prevention.
Second, FOAM ROLLING. Foam rolling has become ubiquitous in running culture, and the research tells a nuanced story. Wiewelhove and colleagues in 2019 conducted a meta-analysis of twenty-one studies and found that foam rolling has, quote, minor and partly negligible effects on performance and recovery. Post-exercise rolling slightly reduces muscle pain perception. Hendricks and colleagues in 2020 found it increases range of motion and may be useful for recovery from exercise-induced muscle damage, with no negative effects on performance.
The honest summary: foam rolling is not harmful, it modestly reduces soreness, and its primary mechanism appears to be neurological, changing pain perception, rather than mechanical, physically breaking up tissue. If it feels good and helps you recover mentally, keep doing it. But it's a complement to strength training, not a substitute for it.
Third, RUNNING SHOES. Perhaps no topic generates more anxiety for new runners than shoe selection. Should you get motion control shoes for overpronation? Maximum cushioning? Minimalist? The evidence may surprise you.
Malisoux and Theisen in 2020 concluded that, quote, the role of running shoe technology in injury prevention has been largely overrated. The traditional paradigm of prescribing shoes based on foot type or pronation pattern is not strongly supported by current research. Napier and Willy in 2022 found that heavily cushioned shoes don't consistently reduce ground reaction forces or injuries, and that controlling pronation doesn't reliably prevent injury either.
What does seem to matter? COMFORT. Malisoux and Theisen introduced the comfort filter paradigm: runners who select shoes based on how they feel, subjective comfort, tend to have fewer injuries than those prescribed shoes based on biomechanical assessments. The practical advice: try on several pairs, run in them briefly if the store allows it, and choose the ones that feel best. Replace them every four hundred to five hundred miles, and don't change shoe type dramatically in the middle of a training cycle.

The Four-Level Framework
Here's a practical framework you can use every time you're uncertain.
Level One, monitor and proceed: Mild, diffuse soreness that's bilateral or that goes away within the first ten minutes of running. This is normal adaptation. Run your planned workout, but pay attention.
Level Two, modify your training: A specific ache that doesn't worsen during the run but doesn't fully disappear either. Run at reduced intensity, shorten the distance, or substitute a cross-training session. Add extra attention to the affected area in your strength routine.
Level Three, take active rest: Pain that causes you to alter your running form, that worsens as you run, or that's present when walking. Take two to three days off from running. Walking and cross-training are fine if pain-free. Then reassess. If it's improved, return at reduced volume. If it's unchanged, escalate.
Level Four, see a professional: Pain that's present at rest, that hasn't improved after three to five days of modified activity, that involves swelling or visible change, or that registers above a six on a zero to ten scale. See a sports medicine physician or physiotherapist. This is not failure, it's smart training.
A Personal Risk Profile
Injury prevention isn't a single strategy, it's a system. And the most effective system is one tailored to your specific risk profile. The strongest predictor of a future running injury is a previous running injury, as Taunton and colleagues noted in 2012. After that, the most significant modifiable risk factors include training load errors, too much too soon, insufficient recovery, lack of strength training, poor sleep, and limited variety in running surfaces.
Being honest about your vulnerabilities allows you to focus your prevention efforts where they'll matter most. The research is clear that the best routine is one you'll actually do, and that means it needs to be short, targeted, and integrated into your existing training schedule. Fifteen minutes, two to three times per week, is enough to provide meaningful protection, as Blagrove and colleagues showed in 2022. Bodyweight exercises are highly effective, and many of the most important runner's strength movements require nothing more than a floor and a wall.
What Comes Back, and When
We'll return to the psychological dimensions of pain and discomfort in Chapter Six, where we'll explore how your mental relationship with suffering affects both your training and your race. And in Chapter Eight, we'll discuss the hardest version of this decision, whether to continue or stop during the marathon itself, when you've invested months of training and every emotional fiber wants to keep going.
For now, the most important takeaway is this: listening to your body is not weakness. It's a SKILL, arguably the most important skill in your marathon journey. The runners who make it to the finish line are not always the ones with the highest pain tolerance or the most aggressive training schedules. They're the ones who learned to distinguish between the voice that says this is hard and the voice that says something is wrong. They're the ones who were brave enough to back off when backing off was the right call.
The body achieves what the mind believes, but only if the tendons can keep up.
The argument of this chapter
That shin that ached at the beginning of this chapter? If it's a diffuse soreness that fades by the time you're warmed up, lace up and go. If it's a sharp, point-specific pain on one side that showed up yesterday too, take the day off and do your strength routine instead. Both decisions are the right one, as long as you made them consciously rather than on autopilot.
Key Takeaways
- Nearly half of all runners experience injuries, but the vast majority are overuse injuries with recognizable early warning signs (Kakouris et al., 2021; Taunton et al., 2012).
- The cardiovascular-musculoskeletal adaptation gap, where your aerobic fitness outpaces your structural readiness, is the primary framework for understanding why overuse injuries occur in beginner runners.
- Pain and discomfort are different: discomfort is diffuse, bilateral, and resolves during or shortly after activity; pain is localized, unilateral, and worsens or persists.
- The five most common beginner injuries — runner's knee, shin splints, Achilles tendinopathy, plantar fasciitis, and I-T band syndrome — all have early warning signs you can learn to recognize.
- Targeted strength training for glutes, hips, core, and calves is the most evidence-supported modifiable strategy for reducing injury risk, especially when performed with proper form (Blagrove et al., 2022; Blagrove et al., 2024).
- Stretching, foam rolling, and running shoe selection are less impactful for injury prevention than most runners believe. Comfort in shoes matters more than correction (Malisoux & Theisen, 2020; Napier & Willy, 2022).
- Use the four-level decision framework — monitor, modify, rest, or seek help — every time you're unsure whether to train through a symptom.
In Chapter 5 — "Fuel, Not Punishment: Eating and Drinking for the Long Run" — we turn to the fuel that powers all of this adaptation: nutrition and hydration. You'll learn why the popular advice about carbo-loading is mostly wrong, what your body actually needs during long training runs, and how to develop a fueling strategy that prevents the dreaded wall at mile twenty. Your muscles can't rebuild what they don't have the raw materials for, and what you eat during this training cycle matters more than you might expect.
References
Blagrove, R. C., Howatson, G., & Hayes, P. R. (2022). Resistance exercise for improving running economy and running biomechanics and decreasing running-related injury risk: A narrative review. Sports Medicine – Open, 8(1), 98.
Blagrove, R. C., Howatson, G., & Hayes, P. R. (2024). Do exercise-based prevention programs reduce injury in endurance runners? A systematic review and meta-analysis. Sports Medicine, 54(3), 641–656.
Hendricks, S., den Hollander, S., Lambert, M., & Brown, J. (2020). A systematic review and meta-analysis of the effects of foam rolling on range of motion, recovery and markers of athletic performance. Journal of Bodywork and Movement Therapies, 24(3), 105–110.
Kakouris, N., Yener, N., & Fong, D. T. (2021). A systematic review of running-related musculoskeletal injuries in runners. Journal of Sport and Health Science, 10(5), 513–522.
Malisoux, L., & Theisen, D. (2020). Can the "appropriate" footwear prevent injury in leisure-time running? Evidence versus beliefs. Journal of Athletic Training, 55(12), 1215–1223.
Napier, C., & Willy, R. W. (2022). Running injury paradigms and their influence on footwear design features and runner assessment methods: A focused review. Frontiers in Sports and Active Living, 4, 815675.
Taunton, J. E., Ryan, M. B., Clement, D. B., McKenzie, D. C., Lloyd-Smith, D. R., & Zumbo, B. D. (2012). Suspected mechanisms in the cause of overuse running injuries: A clinical review. Sports Medicine, 42(3), 153–164.
Wiewelhove, T., Döweling, A., Schneider, C., Hottenrott, L., Meyer, T., Kellmann, M., Pfeiffer, M., & Ferrauti, A. (2019). A meta-analysis of the effects of foam rolling on performance and recovery. Frontiers in Physiology, 10, 376.