The Caffeine Equation
The World's Most Popular Sleep Saboteur
Caffeine doesn't give you energy — it hides your tiredness, then quietly taxes the deepest stage of your sleep.
It's 2:30 in the afternoon, and you're fading. Your eyelids are heavy, your focus is crumbling, and the afternoon stretches ahead like an endless hallway. So you do what roughly 85% of adults worldwide do: you reach for caffeine. Maybe it's a latte, maybe a tea, maybe an energy drink. Within thirty minutes, the fog lifts. You feel sharp again, productive, even energized. The problem seems solved.
That evening, you climb into bed at 11 p.m. You fall asleep without too much trouble. You wake after seven hours. And yet somehow, you feel unrested, groggy, heavy, as if sleep didn't quite do its job. So you reach for that morning coffee a little more eagerly, and by mid-afternoon, the cycle begins again. What's happening behind the scenes is a story of molecular deception: caffeine didn't eliminate your tiredness that afternoon — it hid it. And when you slept, it quietly stole the deepest, most restorative stage of your night. This chapter unpacks how.
From Chapters 1–3 to Your Coffee Cup
Over the first three chapters, you've built a sophisticated model of sleep regulation. In Chapter 1, you learned about Process S, the homeostatic sleep drive that rises the longer you stay awake, like a pressure gauge slowly filling. In Chapter 2, you explored sleep architecture — the structured progression through N1, N2, N3, and REM stages, each serving distinct biological functions. In Chapter 3, you saw how light sculpts your circadian rhythm, the internal clock that tells your body when to sleep. Now we introduce the single most common chemical that disrupts this elegant system: caffeine.
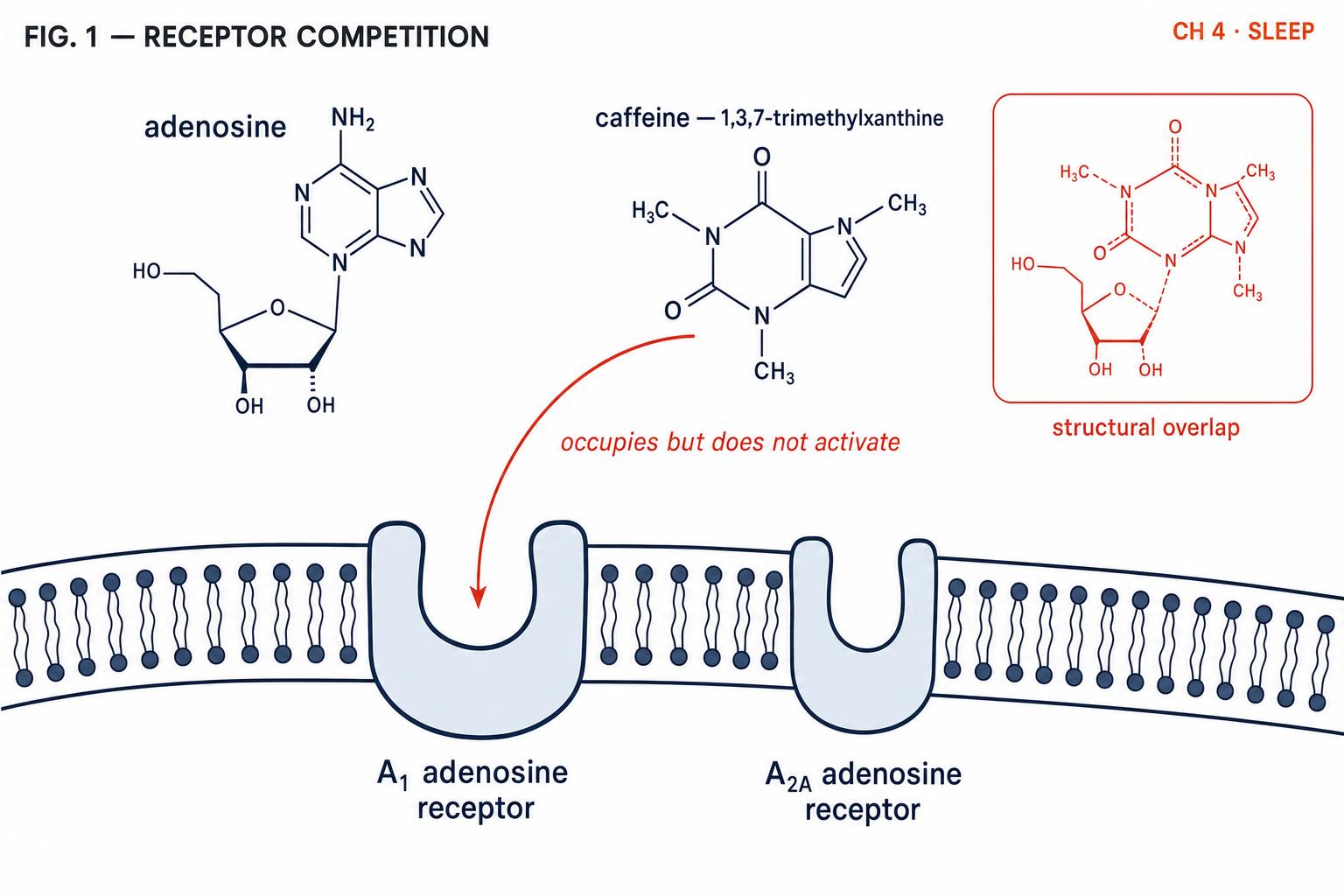
Caffeine is not merely a stimulant in the colloquial sense. It is, with striking molecular precision, an adenosine receptor antagonist — a chemical that targets the exact signaling pathway that Process S relies upon. To understand why your afternoon coffee can silently undermine tonight's sleep, we need to return to the molecule at the heart of sleep pressure: adenosine.
The Adenosine Story — How Your Brain Builds Sleep Pressure
Recall from Chapter 1 that adenosine is a byproduct of neuronal energy metabolism. Every time your brain cells fire — processing information, solving problems, navigating your day — they consume adenosine triphosphate (ATP) for fuel, and adenosine gradually accumulates in the extracellular space. This accumulation is the biological basis of Process S. The longer you're awake, the more adenosine builds up, and the sleepier you feel (Reichert et al., 2022).
Adenosine produces this sensation of drowsiness by binding to specific receptors on the surface of neurons — primarily the A1 receptors, which inhibit wake-promoting neurons, and the A2A receptors, which activate sleep-promoting pathways in the basal forebrain. When adenosine docks into these receptors, it's like turning a dimmer switch: neural activity gradually winds down, arousal decreases, and the brain moves toward a sleep-ready state.
Here is where caffeine enters the picture, and where its mechanism is both elegant and insidious.
A Molecular Game of Musical Chairs
Caffeine's three-dimensional molecular structure is remarkably similar to adenosine. Similar enough, in fact, that caffeine can slide into the same A1 and A2A receptors. But here's the critical difference: caffeine occupies those receptors without activating them. It sits in the chair but doesn't do the job. This is what pharmacologists mean by antagonism — caffeine blocks the receptor without triggering the downstream signal (Reichert et al., 2022).
Imagine a game of musical chairs. Adenosine molecules are the players trying to sit down, and every time one sits, the sleepiness signal gets a little louder. Caffeine molecules are imposters wearing adenosine costumes. They rush in and occupy chairs, preventing real adenosine from sitting. The music keeps playing, the signal stays quiet, and you feel awake. But — and this is the point students often miss — adenosine production doesn't stop. Your brain is still consuming energy, still generating adenosine. The molecules are still accumulating. They just can't get to their chairs.
This is why caffeine doesn't give you energy in any true metabolic sense. It gives you the perception of wakefulness by masking a signal that was telling you the truth: you're tired, and getting more tired by the minute.
The Caffeine Crash, Explained
You already know the answer from experience. When caffeine is eventually metabolised by the liver and its molecules release from the receptors, all of that pent-up adenosine — which has been accumulating for hours — suddenly floods the now-vacant receptors. The dimmer switch doesn't gently descend; it slams down. This is the caffeine crash: not a new wave of tiredness, but the delayed arrival of tiredness that was building all along. The Process S curve didn't flatten while you were caffeinated — it kept rising in the background, invisible. Caffeine merely shifted when you felt it (Reichert et al., 2022).
Caffeine Pharmacokinetics — The Half-Life Problem
Understanding that caffeine masks adenosine is only half the story. The other half is understanding how long it takes your body to clear caffeine, because this determines whether that afternoon coffee is still lingering in your brain at bedtime.
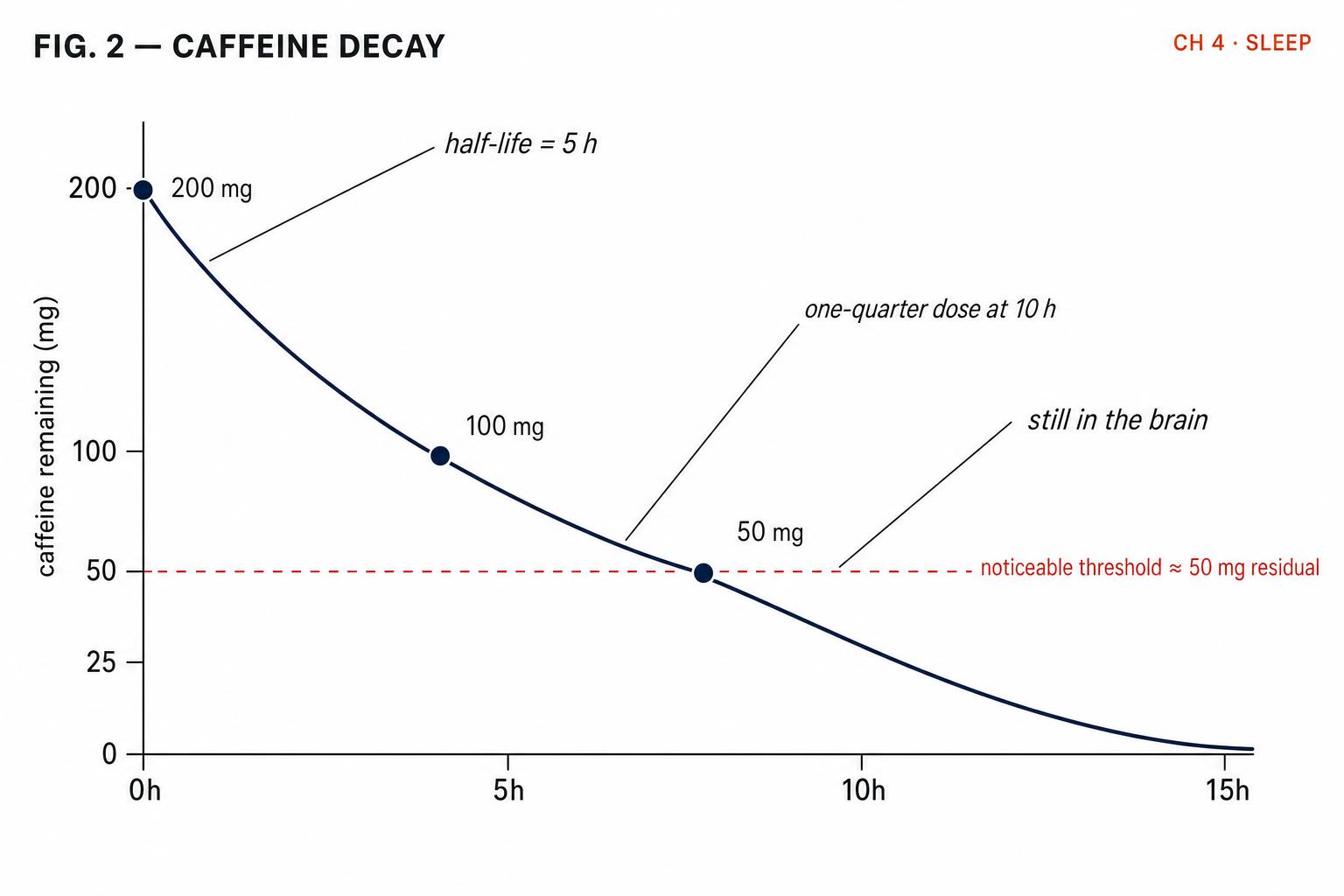
Caffeine is absorbed rapidly through the gastrointestinal tract, reaching peak blood concentration within 30–60 minutes of ingestion. It readily crosses the blood-brain barrier, meaning it reaches your central nervous system quickly and efficiently. But clearing it is a far slower process. The half-life of caffeine — the time it takes for your body to eliminate half of the caffeine in your bloodstream — averages approximately 5 hours in healthy adults, though the range spans from 1.5 to 9.5 hours (Institute of Medicine, 2001).
Let's do some practical arithmetic. Say you drink a standard drip coffee containing 200 mg of caffeine at 2 p.m. With a 5-hour half-life: by 7 p.m., 100 mg is still circulating — half the original dose. By midnight, approximately 50 mg remains — one quarter. By 5 a.m., approximately 25 mg is still present — one eighth. That single afternoon coffee has measurable caffeine levels in your brain well into the early morning hours. And if you had two coffees, or added an energy drink, the numbers stack up. Caffeine from multiple doses accumulates, and each dose decays on its own timeline.
Why Your Half-Life Isn't Average
The 5-hour average conceals enormous individual variation, and this variation is largely determined by the CYP1A2 enzyme in your liver — the enzyme responsible for metabolising approximately 95% of ingested caffeine (Nehlig, 2018). Your CYP1A2 gene comes in different variants, and these variants produce dramatically different metabolic speeds.
Fast metabolisers carry gene variants that produce highly active CYP1A2 enzymes. Their half-life may be as short as 2–3 hours. Slow metabolisers carry less active variants and may have half-lives of 7–9 hours — meaning caffeine lingers in their system nearly three times longer. In genetic knockout studies, mice lacking CYP1A2 entirely showed caffeine half-lives seven times longer than normal, confirming this enzyme as the critical bottleneck (Berthou et al., 1996).
But genetics isn't the only factor. Several conditions and substances alter caffeine metabolism significantly (Institute of Medicine, 2001; Nehlig, 2018): oral contraceptives can approximately double caffeine half-life; pregnancy extends half-life dramatically — up to 15 hours in the third trimester; smoking accelerates CYP1A2 activity, shortening half-life (which is why smokers often drink more coffee); age — older adults generally metabolise caffeine more slowly; and liver disease can extend half-life substantially.
This variation explains a frustrating reality: generic advice like "no coffee after 2 p.m." is reasonable for average metabolisers but may be too permissive for slow metabolisers and unnecessarily restrictive for fast ones. The right answer depends on your biology.
The Deep-Sleep Tax — What Caffeine Really Steals
Here is where the caffeine story takes its most consequential turn, and where many people's confidence that "coffee doesn't affect my sleep" starts to crumble.
In a landmark study, Drake and colleagues (2013) gave participants 400 mg of caffeine at three different times: immediately before bed, three hours before bed, and six hours before bed. The results were striking: even caffeine consumed six hours before bedtime reduced total objective sleep time by more than one hour. But the truly remarkable finding was this: participants themselves did not perceive the disruption. Their subjective reports of sleep quality remained largely unchanged even as their polysomnography readings told a very different story.
This disconnect between subjective experience and objective measurement is one of the most important takeaways from this chapter. And it becomes even more concerning when we examine which part of sleep caffeine targets.
Caffeine's Selective Attack on N3 Slow-Wave Sleep
A comprehensive meta-analysis by Gardiner and colleagues (2023) synthesised data across multiple studies and found that caffeine produces significant dose-dependent reductions in N3 (slow-wave) sleep — an average reduction of 11.4 minutes in absolute N3 time. Four studies additionally found significant reductions in delta-frequency EEG power during NREM sleep, confirming that it's not just time in N3 that decreases but the depth and intensity of slow-wave activity.
This matters enormously because, as you learned in Chapter 2, N3 is the stage most associated with physical restoration, growth hormone release, immune function, and the glymphatic clearance of metabolic waste — including beta-amyloid, a protein implicated in Alzheimer's disease. N3 is concentrated in the first two sleep cycles, which is precisely the period when residual caffeine levels are highest if consumed in the afternoon or evening.
Perhaps the most striking demonstration comes from the classic study by Landolt and colleagues (1995), who showed that caffeine administered at 7:10 in the morning — roughly 16 hours before sleep onset — still significantly reduced sleep efficiency and delta-frequency power during nighttime sleep. Even at a dose of just 200 mg (roughly two cups of coffee), and even when salivary caffeine levels had declined to very low concentrations by bedtime, the residual impact on slow-wave sleep architecture was measurable.
A more recent randomised clinical trial reinforced these findings. Gardiner and colleagues (2025) demonstrated that 400 mg of caffeine consumed within 12 hours of bedtime significantly reduced N3 sleep, noting "the potent ability of caffeine to reduce N3 sleep." Critically, they found that while our brains normally protect N3 sleep even during sleep restriction — treating it as the highest priority stage — caffeine overrides this protective mechanism. The one reassuring finding: a 100 mg dose (roughly one cup of tea or a small coffee) did not produce significant N3 disruption.
"But Coffee Doesn't Affect My Sleep"
This is the most common objection students — and adults generally — raise when presented with caffeine-sleep research. And on the surface, it seems like a reasonable claim. Many people drink coffee late in the day, fall asleep without difficulty, and wake up after seven or eight hours.
The study by Drake and colleagues (2013) directly addresses this. Participants who consumed 400 mg of caffeine six hours before bed reported subjective sleep quality that was essentially unchanged from placebo nights — yet polysomnography revealed they lost more than an hour of total sleep and experienced significantly altered sleep architecture. The participants were, in a very real sense, unaware of the damage.
Subjective reports of sleep quality are unreliable indicators of caffeine-induced sleep disruption. Individuals consistently underestimate the effects of caffeine on their sleep when compared to objective polysomnographic measures.
Drake et al., 2013
There are several reasons for this perceptual blindness. First, sleep onset may be unaffected — caffeine's primary impact is on sleep architecture, not necessarily sleep latency. You can fall asleep on schedule and still lose deep sleep. Second, we don't perceive sleep stages. You cannot consciously tell the difference between a night of robust N3 sleep and one where N3 was curtailed by 30%. The experience of sleeping feels similar either way. Third, chronic caffeine use resets your baseline. If you drink caffeine daily, you may have never experienced your true sleep architecture as an adult. What feels normal may already be a caffeine-degraded version of your potential sleep quality. Fourth, tolerance masks some wakefulness effects but does not eliminate the sleep-architecture disruption. Regular caffeine users develop tolerance to the subjective alerting effects, but research suggests the N3-suppressing effects persist (Reichert et al., 2022).
The implication is both humbling and empowering. Humbling because it means our intuitions about our own sleep are less reliable than we'd like. Empowering because it suggests that, for many people, a simple adjustment to caffeine timing could unlock meaningfully better sleep — without sleeping more hours, just sleeping more deeply.
Building Your Personal Caffeine Cutoff
Armed with the pharmacology, the individual variation data, and the sleep architecture research, you can now approach caffeine with a degree of precision that most people never apply. The goal isn't necessarily to eliminate caffeine. It's to align your consumption with your biology so that caffeine serves you during the day without sabotaging you at night.
A reasonable heuristic is to ensure that your blood caffeine level is below approximately 100 mg equivalent by bedtime. Gardiner et al. (2025) found that 100 mg doses did not produce significant N3 disruption, while 400 mg doses consumed within 12 hours did. Working backward from your bedtime using your estimated half-life:
- Fast metabolisers (≈ 3 h half-life): a 200 mg coffee at 4 p.m. drops to around 50 mg by 10 p.m. — likely acceptable for an 11 p.m. bedtime.
- Average metabolisers (≈ 5 h half-life): the same 200 mg coffee at 4 p.m. is still around 80 mg at 10 p.m. and around 50 mg at midnight. A noon cutoff for larger doses is safest.
- Slow metabolisers (≈ 7.5 h half-life): 200 mg at noon is still around 100 mg at 7:30 p.m. and around 50 mg at 3 a.m. A morning-only policy may be necessary.
If you don't know your metabolizer type, several clues can help. Do you feel wired for hours after a single coffee? You may be a slow metaboliser. Can you drink espresso at dinner and fall asleep easily? You may be fast — though remember, falling asleep easily doesn't mean your deep sleep is unaffected. Are you taking oral contraceptives, are you over 60, or do you have liver concerns? Factor in a longer half-life.
Connecting Back to the Two-Process Model
The beauty of understanding caffeine through the lens of Process S is that it demystifies both its appeal and its risks. Caffeine doesn't give you extra wakefulness — it borrows it from your homeostatic sleep drive, then charges interest in the form of degraded deep sleep. Process S rises linearly during wakefulness. Caffeine doesn't change that line; it merely hides it from your conscious experience while it keeps climbing. The crash, when it comes, is the moment the mask slips and the true height of the curve becomes apparent.
Meanwhile, caffeine also interacts with Process C, the circadian system. Caffeine consumed in the evening can delay the timing of melatonin release — much like the evening light exposure discussed in Chapter 3 — further pushing your circadian clock later and making it harder to fall asleep at your intended time. The two-process model thus becomes a framework for understanding not just why caffeine keeps you awake, but why it fragments your sleep even when it doesn't prevent it.
Key Takeaways
- Caffeine is an adenosine receptor antagonist. It blocks the A1 and A2A receptors without activating them, masking sleepiness without reducing the underlying sleep pressure.
- Adenosine continues to accumulate during caffeine use; when caffeine is metabolised, the pent-up adenosine floods receptors, causing the caffeine crash.
- Caffeine's half-life averages around 5 hours but ranges from 1.5 to 9.5 hours, driven primarily by CYP1A2 genetics — with oral contraceptives, pregnancy, age, and liver health as additional factors.
- Caffeine disproportionately reduces N3 slow-wave deep sleep — even when total sleep duration appears normal — by an average of around 11 minutes, with greater effects at higher doses and later timing (Gardiner et al., 2023).
- Subjective sleep quality is a poor indicator of caffeine's impact; people consistently underestimate the disruption measured by polysomnography (Drake et al., 2013).
- Personalised caffeine cutoffs should account for individual metabolism, total daily intake, and the goal of reaching approximately 100 mg or less circulating caffeine by bedtime.
- Caffeine tolerance reduces the perceived alerting effects but does not eliminate sleep-architecture disruption (Reichert et al., 2022).
Now that you understand how caffeine masks the homeostatic sleep signal, Chapter 5 — Moving to Sleep: Exercise, Body Temperature, and the Gate to Slumber — explores the other half of the equation: how movement and core body temperature shape the descent into deep sleep, and why the timing of exercise can either widen or jam shut your nightly sleep gate.
References
Berthou, F., Flinois, J. P., Ratanasavanh, D., Beaune, P., Riche, C., & Guillouzo, A. (1996). Role of CYP1A2 in caffeine pharmacokinetics and metabolism: Studies using mice deficient in CYP1A2. Pharmacogenetics, 6(4), 291–296.
Drake, C., Roehrs, T., Shambroom, J., & Roth, T. (2013). Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. Journal of Clinical Sleep Medicine, 9(11), 1195–1200.
Gardiner, C., Weakley, J., Burke, L. M., Roach, G. D., Sargent, C., Maniar, N., Townshend, A., & Halson, S. L. (2023). The effect of caffeine on subsequent sleep: A systematic review and meta-analysis. Sleep Medicine Reviews, 69, 101764.
Gardiner, C., Weakley, J., Janssen, X., Roach, G. D., Sargent, C., Maniar, N., Townshend, A., & Halson, S. L. (2025). Dose and timing effects of caffeine on subsequent sleep: A randomized clinical crossover trial. Sleep, 48(4), zsae230.
Institute of Medicine (US) Committee on Military Nutrition Research. (2001). Pharmacology of caffeine. In Caffeine for the sustainment of mental task performance: Formulations for military operations. National Academies Press.
Landolt, H. P., Werth, E., Borbély, A. A., & Dijk, D. J. (1995). Caffeine intake (200 mg) in the morning affects human sleep and EEG power spectra at night. Brain Research, 675(1–2), 67–74.
Nehlig, A. (2018). Interindividual differences in caffeine metabolism and factors driving caffeine consumption. Pharmacological Reviews, 70(2), 384–411.
Reichert, C. F., Deboer, T., & Landolt, H. P. (2022). Adenosine, caffeine, and sleep–wake regulation: State of the science and perspectives. Journal of Sleep Research, 31(4), e13597.